

American College of Cardiology’s New Long-Term Approach to Cholesterol Management Shaped by Work of MSU’s Chaz Hong
April 15, 2026
Why this matters:
- A landmark update to cholesterol guidelines cites a 2020 paper co-authored by Charles (Chaz) Hong, MD, PhD, chair of Michigan State University College of Human Medicine Department of Medicine.
- The guidelines emphasize much earlier screening and intervention — including medication — to control cholesterol and risk of heart disease.
- Hong, a cardiologist and researcher, says the guidelines have the potential to save millions of lives.

Charles (Chaz) Hong, MD, PhD, heard the skepticism from some patients when he counseled them about a proven, inexpensive way to control cholesterol and prevent heart disease, the No. 1 cause of death and disability.
“Literally, I would prescribe statins, and half the people would say, ‘I don't want to take it,’” said Hong, a Michigan State University College of Human Medicine cardiologist, researcher and chair of the Department of Medicine. “You have to actually negotiate with patients to have them take statins, which is strange, because statins have saved hundreds of millions of lives.”
Hong, whose email signature reads, “All cures — past, present & future — come from research,” took that skepticism as motivation to investigate the value of early intervention for heart disease.
Now a 2020 paper he co-authored has been instrumental in a landmark set of guidelines recently issued by The American College of Cardiology and the American Heart Association.
The guidelines emphasize keeping cholesterol levels lower for longer. This requires screening and intervention at a younger age, including considering the use of statins when diet, exercise and lifestyle changes are insufficient.
The risk of long-term exposure to cholesterol was a key point examined in Hong’s paper, Time Course of LDL Cholesterol Exposure and Cardiovascular Disease Event Risk, which is cited several times in the new guidelines. Though he worked on the paper before his arrival at MSU, the impact of the findings endures.
According to the American College of Cardiology, 1 in 4 U.S. adults has high levels of low-density lipoprotein-cholesterol (LDL-C), often called “bad cholesterol.” A buildup of fatty deposits in the arteries can increase the risk of stroke or heart attack.
“When I was in medical school, LDL-C of 130 mg/dL (milligrams per deciliter) was considered normal or even desirable. But nature told us this probably wasn’t,” Hong said. He cited examples from several studies:
- The average LDL-C of a newborn is 30 to 50 mg/dL, suggesting this is our “natural state,” prior to dietary influences.
- The lowest recorded prevalence of coronary atherosclerosis — the buildup of plaque in the coronary arteries — was among the forager horticulturalist tribes of the Bolivian Amazon. They have an LDL-C of 70 to 90 mg/dL.
- People who carry loss-of-function mutations in the PCSK9 gene, involving LDL-receptor degradation, had almost 90% lower risk of coronary heart disease even though their cholesterol reduction was rather modest at about 28%.
- The Framingham Offspring Study found that being diagnosed with high cholesterol at 45 years old put one at higher risk for developing heart disease than being diagnosed at 55.
What Hong’s paper found was that the exposure to high cholesterol happening over a lifetime can be a better measure of long-term risk than a snapshot of cholesterol level later in life. For example, someone whose LDL-C levels are higher at a younger age, as young as 18 to 30 years old, would be at greater risk than someone whose LDL-C reached the same level at a later age.
“Our conclusion was that we’re starting cholesterol monitoring and control way too late, because heart disease doesn't occur overnight,” Hong said. “It happens over decades.”
The findings helped inform a new cardiovascular risk calculator, Predicting Risk of Cardiovascular Disease EVENTS (PREVENT), which is included in the new guidelines.
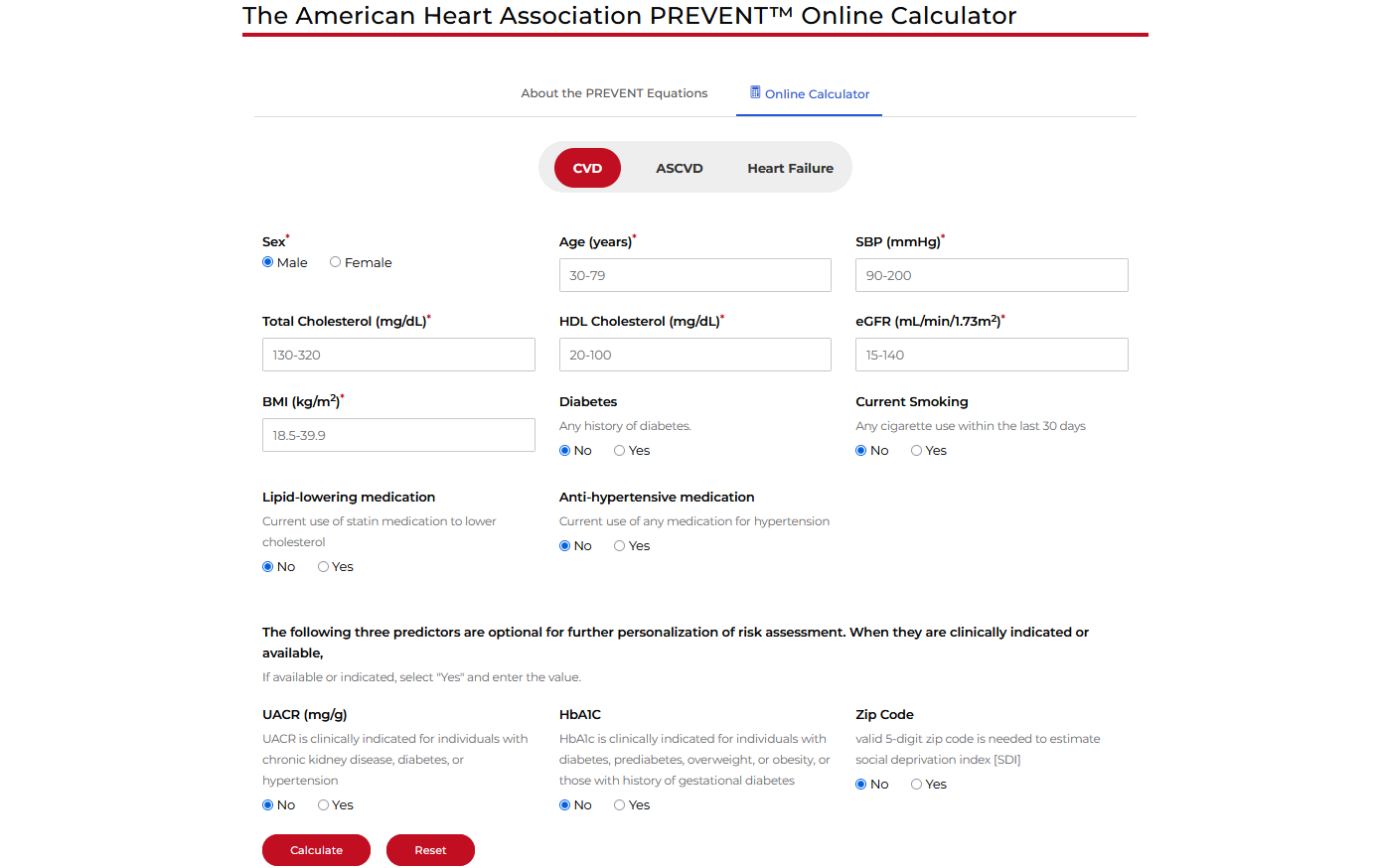
“Rather than just a 10-year window and then trying to be really aggressive on people who already have the disease, now we’re looking at a 30-year window,” Hong said. “The new calculator promotes earlier intervention of the drugs, instead of starting when it’s already too late.”
Roger Blumenthal, MD, director of the Johns Hopkins Ciccarone Center for the Prevention of Heart Disease, who chaired the guideline writing committee, said the PREVENT calculator provides a simple process to assess risk. Blood samples can be drawn during primary care visits, even starting in childhood. If levels remain high into a patient’s 30s, medications such as statins could be considered.
“We always want to encourage lifestyle improvements, but the judicious use of medication can be beneficial,” Blumenthal said. “What I find most useful with the PREVENT scores is the estimation of longer risk if they don't make any changes.”
And patients can have confidence in the science behind the new guidelines, he said.
“Many Americans are used to taking unproven supplements, yet they have a hard time considering a proven medication. It's a free country, but the job of clinicians is to motivate patients to make evidence-based choices,” Blumenthal said.
“We have such overwhelming data that Chaz and others have contributed to show that lower LDL for longer is better.”
Hong said it’s important for people to understand that the new guidelines are based on decades of science, because they could help save millions of lives.
“If we actually have people adopt this practice, start statins in their 30s and 40s when appropriate, then I think that we could dramatically reduce the rate of stroke and heart attacks in 30 years. I'm very excited that this has the potential to save a lot of lives,” he said, acknowledging he will still encounter skeptics.
“So when I recommend this to my patients,” he said, “what I tell them is that ‘This is not going to save your life now, but it's going to help you have a long and healthy retirement.’"
By Darin Estep
Media Contact | Emily Linnert